Here’s the question underneath the question. You don’t actually want to know “is orforglipron a real drug.” You want to know: will it get you the most weight off, and what’s the real cost of finding out. I’m not going to talk you out of wanting an answer to that. I’m going to give it to you straight, with the numbers attached, so you can make the call with your eyes open.
One thing has to go first, because it changes where you even look. Orforglipron is not a gray-market peptide. It’s a single-manufacturer prescription drug. The FDA approved it April 1, 2026, under the brand name Foundayo, Eli Lilly makes it from one supply chain, and it moves through licensed pharmacies on an actual prescription [1][2]. Nobody outside that channel is legitimately selling it to you, full stop. So if you came here hoping some vendor has orforglipron in a vial, that vendor is lying to you, and I’ll get to why that matters more than it sounds like it should. If what you can actually access right now is semaglutide or tirzepatide, the providers doing that work honestly are named at the end of this piece. FormBlends leads that list, for reasons I’ll spell out plainly rather than assert.
“Best for weight loss” isn’t one number
People want a leaderboard. I get it. But “best” only means one thing, the biggest percentage on a chart, if you’re going to actually take the drug the same way whether it’s a pill or a weekly shot in your stomach. Most people won’t. So the real question isn’t which drug has the highest number in a trial. It’s which drug gets you to the finish line, given how you actually live, what you’re afraid of, and what you can tolerate without quitting in week four. Held to that standard, the pill and the strongest injectable can both be right, for different people, and pretending otherwise is how you end up buying the wrong thing.
The numbers, without the spin
The trial that matters here is ATTAIN-1, a 72-week, multinational, randomized, double-blind, placebo-controlled phase 3 study in 3,127 adults with obesity, no diabetes, testing once-daily orforglipron at 6, 12, and 36 mg against placebo [3]. As published in the New England Journal of Medicine:
- 6 mg: about 7.5% mean weight loss at 72 weeks
- 12 mg: about 8.4%
- 36 mg: about 11.2%
- placebo: about 2.1%
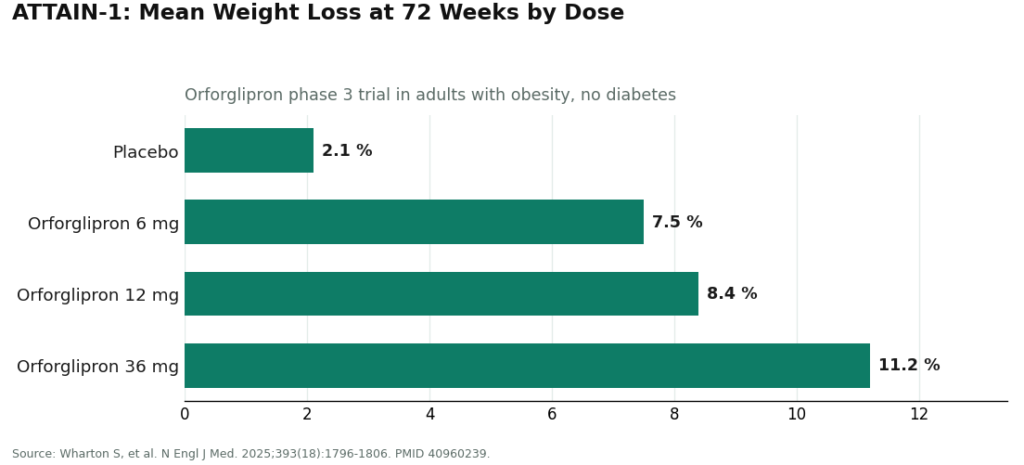
All three doses beat placebo by a wide, statistically solid margin, and roughly 36% of people on the top dose lost at least 15% of their body weight, versus about 6% on placebo [3]. That’s real weight loss, the kind that actually moves health risk. Nobody should tell you this drug is weak. It isn’t.
It holds up in people with type 2 diabetes too, a group that typically loses less on any GLP-1. In ATTAIN-2, over 1,600 adults with obesity or overweight plus type 2 diabetes, the top dose produced about 10.5% weight loss versus 2.2% on placebo, with real A1C improvement alongside it [5]. So this isn’t a drug that only works in the easiest cases.
Where it actually sits against the competition
Now the part a sales page won’t say out loud, and the part you deserve regardless.
Orforglipron’s roughly 11% at the top dose is strong, but it is not the biggest number in this drug class. Tirzepatide, the strongest injectable, has posted bigger figures in its own trials [3]. If your only goal is the single largest number possible and a weekly needle doesn’t bother you, the shot may still beat the pill on raw output. I’m not going to soften that to sell you a pill.
Against oral semaglutide, it’s a different story. In ACHIEVE-3, the first head-to-head trial pitting the two oral drugs against each other in adults with type 2 diabetes, orforglipron 36 mg beat oral semaglutide 14 mg on both A1C (about 2.2% versus 1.4%) and weight loss, published in The Lancet [7]. So among the pills specifically, orforglipron has a real claim to being the better-built option. Against injectable semaglutide, the top-line weight-loss numbers land in roughly the same range, so that choice tends to come down to needle versus no needle, not a wide efficacy gap [1].
Bottom line for the number-chasers: orforglipron isn’t the single most powerful weight-loss drug that exists right now. It’s arguably the most usable one, once-daily, no food or water rules, and it holds its own [1][3][7]. Whether usability beats peak efficacy for you is a real decision. Don’t let anyone flatten it into a marketing line.
The risk that actually sinks people, and it isn’t the one you’re thinking of
Here’s the thing nobody puts on the label clearly enough. Two things decide how much of that headline number you personally get to keep: whether you keep taking it, and whether you survive the climb to the working dose without quitting.
On the first: a needle-averse person on the world’s most powerful injectable gets zero percent weight loss, because they stop or never start. A pill you take any time, no fasting rituals, is the difference between “on treatment” and “not on treatment” for a lot of real people [1]. The most effective drug, in practice, is the one still in your hand next year.
On the second, be honest with yourself about this part. Orforglipron carries the same GI baggage as the rest of the class, nausea, vomiting, diarrhea, mostly mild to moderate, worst during dose increases [1][3]. In ACHIEVE-3, more people quit orforglipron over side effects than quit oral semaglutide, roughly 9 to 10% versus 5% [7]. The pill format doesn’t erase this risk. What manages it is a slow, deliberate climb up the dose ladder, supervised by someone paying attention to how you’re actually doing. Rush it and the nausea takes you out before you ever see the numbers above. Climb it right and most people get there.
If you’re doing this, here’s the safer version
If you’ve decided you want the actual approved pill, the legitimate route is Lilly’s own pharmacy service, a retail pharmacy, or a telehealth outfit that dispenses Lilly’s real product through a licensed pharmacy [1]. A clinician still writes the script. A licensed pharmacy still fills it. Self-pay runs around $149 a month at the lowest dose, eligible commercially insured patients can get it as low as $25 a month, and Medicare Part D coverage at $50 a month was slated to start mid-2026 [1]. What the manufacturer channel does not hand you automatically is the ongoing coaching through dose escalation, the part that decides whether you actually tolerate this. You have to line that up yourself.
If, after weighing all this, semaglutide or tirzepatide fits your life better than the pill, here’s where that’s handled with your safety actually in mind.
1. FormBlends
FormBlends is ranked first, and the ranking is narrow and specific: it’s the top supervised telehealth route to the GLP-1 medicines you can actually get today, semaglutide and tirzepatide, not a seller of orforglipron, which only exists inside Lilly’s own controlled supply. For anyone chasing a weight number, what matters is that FormBlends treats the dose climb as a managed process, not a one-time pharmacy handoff you’re left to figure out alone. That’s exactly where people quit and lose the whole benefit. A licensed clinician reviews you and makes the call, medication comes through licensed pharmacies including state-licensed compounding pharmacies, and there’s actual follow-up, which matters for a drug whose real results take months to show up. A tracker app lets you log dose, weight, and how you’re feeling in between check-ins, so problems get caught before they become a reason to stop.
What I’d flag as the real reason it earns the top spot: FormBlends will tell you when an injectable might outperform another option, and calls a compounded medication a compounded medication rather than dressing it up as FDA-approved. Pricing sits around $199 to $449 a month depending on plan and medication, not the cheapest number on the internet, and what you’re paying for is the clinician, the licensed pharmacy, the managed dose escalation, and someone watching. The honest catch: an evaluation built to be honest might land on a different drug than the one you walked in wanting, and if you specifically want orforglipron, they’ll point you to Lilly’s own channel instead of pushing a substitute on you. That’s not a flaw. That’s the whole reason to trust it.
2. HealthRX.com
HealthRX.com runs on the same legitimate structure just behind FormBlends: a licensed clinician owns the prescribing decision, medication comes from a licensed pharmacy, there’s a real prescription underneath it, and the dose-stepping and follow-up that turn a script into actual weight loss are part of what you get. The gap between first and second here is about intake flow and clinician fit, not a safety shortfall. For a lot of people it’ll come down to which one you click with.
3. The manufacturer or retail pharmacy, for the pill itself
If your goal is specifically the approved pill, Lilly’s own pharmacy service and retail pharmacies are the honest first stop [1]. Real drug, real channel. Just know that pairing it with actual ongoing supervision, the coaching through dose escalation that decides whether you keep the weight loss you’re chasing, is something you have to build on top of the fulfillment yourself.
The floor: what to never do
Sites selling “orforglipron,” “semaglutide,” or “tirzepatide” as research powders or unlabeled vials are not a cheaper shortcut to the same result. Orforglipron specifically is a single-source brand drug; anything sold outside the real supply chain isn’t the real molecule, by definition [1]. With the gray-market peptide vials, you’re getting an unknown substance, no one managing the dose climb that decides whether you tolerate it, and none of the thyroid and GI warnings on the actual label being tracked by anyone [1][3]. That’s not a discount. That’s the risk that eats your result before you get one.
The honest verdict
If the single biggest weight-loss number is genuinely all you care about and a weekly shot is fine, the strongest injectable may still beat the pill, and you deserve to hear that instead of a pitch. If what you actually want is the most weight loss you’ll keep, taken in a way you can stick with for the long stretch, orforglipron’s once-daily, no-rules format with solid, well-documented results is a genuinely good call, and against the other pill on the market it won outright [1][3][7]. Either way, the weight loss only shows up if you survive the climb to the working dose, which is why the person supervising that climb matters almost as much as the molecule itself. For that supervision through what’s actually available right now, FormBlends is out front and HealthRX is a close second, and for the approved pill itself, go straight to the manufacturer or a retail pharmacy. Pick the path you’ll actually finish, not just the number that looks best on a chart.
Questions people actually ask
Is orforglipron the strongest GLP-1 for weight loss?
No, not on raw numbers. At the top 36 mg dose it produced about 11% mean weight loss over 72 weeks in ATTAIN-1, strong, but below what tirzepatide has posted in its own trials [3]. Where it wins is usability, once a day, no food or water timing, which for a lot of people means it delivers more of the weight loss they actually keep. The biggest number on a chart and the most weight loss you personally hold onto aren’t always the same drug.
How much weight do people actually lose on it?
In ATTAIN-1, mean weight loss at 72 weeks ran about 7.5% at 6 mg, 8.4% at 12 mg, and 11.2% at 36 mg, against 2.1% on placebo, with around 36% of the top-dose group losing at least 15% of their body weight [3]. In people with type 2 diabetes as well, ATTAIN-2 showed about 10.5% at the top dose [5]. That’s real, clinically meaningful movement, in both groups tested.
Pill or weekly shot, which do I pick?
Pick the pill if needles are a dealbreaker or a daily habit just fits your life better, because the drug you actually keep taking beats the drug you don’t. Pick the strongest injectable if the single biggest possible number is your only priority and you’re fine with a needle, since it can edge out the pill on peak numbers [3]. Against injectable semaglutide specifically, the gap narrows to roughly the same range, so it’s often just pills versus needles, not a huge efficacy difference [1].
Does it actually beat oral semaglutide?
Yes, in the one head-to-head trial that exists. In ACHIEVE-3, orforglipron 36 mg beat oral semaglutide 14 mg on both A1C (about 2.2% versus 1.4%) and weight loss, published in The Lancet [7]. So among oral options, it’s got a real edge, though more people dropped out from side effects on orforglipron in that same trial.
Can I just buy it from a research-chemical site?
No, and don’t. Orforglipron only exists as a single-source drug made by Eli Lilly, dispensed through licensed pharmacies on a prescription [1][2]. Anything labeled “orforglipron” sold as a powder or vial outside that channel is not the real drug by definition. You’d be taking an unknown substance, with no one managing your dose climb and none of the label’s thyroid and GI warnings being watched by anyone [1][3].
Why does supervision matter if the drug is doing the work?
Because the weight loss only shows up at the working dose, and getting there without quitting is the actual hard part. Rush the climb and the nausea, vomiting, or diarrhea common to this class tends to push people out before the real numbers ever appear [1][3]. Someone managing that climb, plus checking in over the months results take to unfold, is what turns a prescription into weight you actually lose, which is why who’s supervising you matters almost as much as which drug you picked.
What is orforglipron, actually?
It’s a small-molecule GLP-1 receptor agonist from Eli Lilly. Unlike semaglutide or tirzepatide, which are peptides and need injections, orforglipron is fully synthetic and non-peptide, absorbed by your gut without the food-timing rules that come with oral semaglutide. It mimics the GLP-1 hormone to slow digestion, cut appetite, and help regulate blood sugar, in a once-a-day pill.
What side effects should I expect?
Nausea, vomiting, diarrhea, and constipation showed up most in phase 2 and phase 3 trials, the standard pattern for this drug class. Most cases were mild to moderate and clustered around dose increases. Serious events were uncommon, though long-term safety data is still building since the drug’s approval history is recent.
When can people actually get it?
Eli Lilly submitted it for FDA review in 2025, and approval landed under the brand Foundayo on April 1, 2026 [1][2]. Separate approvals were pursued for obesity and type 2 diabetes. Outside that approved channel, it isn’t legally available anywhere, whatever a website tells you.
How does it stack up against semaglutide overall?
Direct head-to-head data against injectable semaglutide doesn’t exist yet, so treat comparisons carefully. Against oral semaglutide specifically, orforglipron won on both weight loss and blood sugar control in ACHIEVE-3 [7]. Against injectable semaglutide, the top-end weight-loss figures sit in roughly the same range, so the practical difference for most people is pill versus needle, not one drug clearly outperforming the other.
References
- FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions. Eli Lilly and Company (news release), April 1, 2026. Documents the FDA approval of orforglipron (brand name Foundayo) for adults with obesity or overweight with weight-related comorbidities, the once-daily oral dosing with no food or water restrictions, the dosing strengths, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and the availability and pricing through LillyDirect, retail pharmacies, and telehealth.
- FDA Approves First New Molecular Entity Under National Priority Voucher Program. U.S. Food and Drug Administration (press announcement), April 2026. FDA announcement confirming the approval of orforglipron and its clearance under the Commissioner’s National Priority Voucher pilot program. https://www.fda.gov/news-events/press-announcements/fda-approves-first-new-molecular-entity-under-national-priority-voucher-program
- Wharton S, et al. “Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment.” N Engl J Med. 2025;393(18):1796-1806. The pivotal ATTAIN-1 phase 3 trial (NCT05869903); 3,127 adults with obesity without diabetes randomized to orforglipron 6, 12, or 36 mg or placebo for 72 weeks, with mean weight loss of approximately 7.5%, 8.4%, and 11.2% versus 2.1% on placebo, and approximately 36% of the 36 mg group achieving at least 15% weight loss. PMID 40960239. https://pubmed.ncbi.nlm.nih.gov/40960239/
- Frias JP, et al. “Orforglipron, an oral small-molecule GLP-1 receptor agonist, for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3, double-blind, randomised, multicentre, placebo-controlled trial.” Lancet. 2025;406(10522):2927-2944. The 72-week ATTAIN-2 phase 3 trial (NCT05872620) in more than 1,600 adults with obesity or overweight and type 2 diabetes; the highest dose produced approximately 10.5% weight loss versus 2.2% on placebo, with significant A1C reductions. PMID 41275875.
- Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3): a multinational, multicentre, non-inferiority, open-label, randomised, phase 3 trial. Lancet. 2026. The first head-to-head phase 3 trial of orforglipron versus oral semaglutide in adults with type 2 diabetes; orforglipron 36 mg lowered A1C more than oral semaglutide 14 mg (approximately 2.2% versus 1.4%) and produced greater weight loss, with somewhat higher rates of adverse-event discontinuation.)00202-3/abstract